You would think a drug that produces real numbers wouldn’t need a sales pitch. That’s exactly why I got suspicious the moment I saw how tirzepatide gets marketed online. When something genuinely works, the people selling it around the edges of the legitimate system don’t stop lying to you. They just change what they lie about. Instead of inflating the results, they start hiding the parts of the label that would make you ask questions.
I spent time with the actual documents on this one: the New England Journal of Medicine trial, the FDA label on DailyMed, the pharmacology entry on the NCBI Bookshelf. I wanted to know what’s real and what’s been quietly sanded off before it reaches you. Here’s what I found, and here’s how they get you.
The trap: a real result, sold with the fine print missing
Tirzepatide is a once-weekly injectable sold under two brand names, Mounjaro for type 2 diabetes and Zepbound for chronic weight management. Same molecule, different FDA approval, different box. It’s a dual agonist, meaning it switches on two gut-hormone receptors instead of one: GLP-1, which older drugs in this category already use, and GIP, a second incretin receptor that most competitors don’t touch [P3]. It’s built as a 39-amino-acid analog engineered to keep both signals active far longer than your body’s own hormones manage on their own, and the downstream effect is documented, not guessed at: more glucose-dependent insulin release, slower stomach emptying, less appetite [P3].
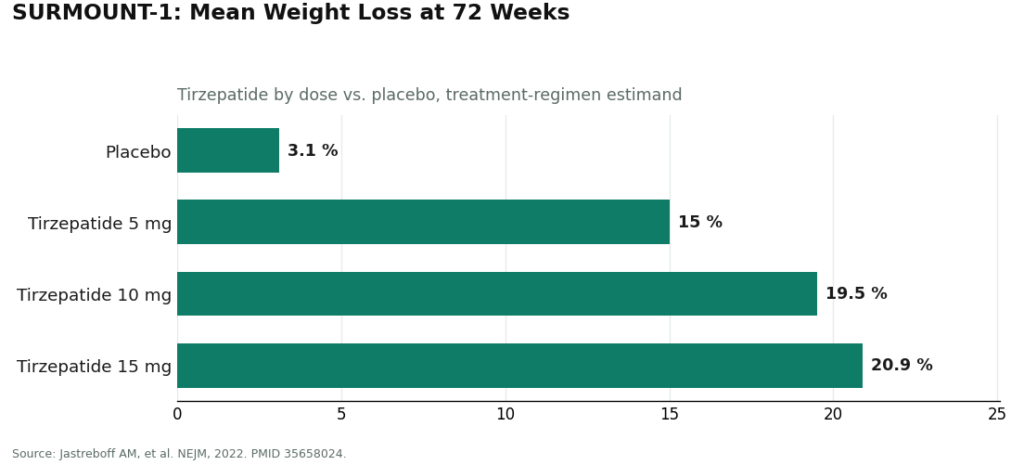
Here’s the part that should stop you in your tracks: the trial numbers are big enough that nobody needs to lie about them, and that’s precisely the danger. SURMOUNT-1, the phase 3 trial published in NEJM in 2022, randomized adults with obesity or overweight to tirzepatide or placebo, with lifestyle support given to both groups, over 72 weeks. Mean weight loss came in around 15.0% at the 5 mg dose, 19.5% at 10 mg, and 20.9% at the 15 mg dose, against roughly 3.1% for placebo [P1]. Those are the conservative, everyone-counted figures, not some cherry-picked best-case subgroup.
That real number, 20.9%, is exactly what a bad actor wants sitting next to their product, because it does the persuading for them. Nobody needs to round it up to 25%. They just need you to forget everything that comes attached to it.
How to spot the tricks
Trick one: they let you assume the average is a guarantee. The 20.9% figure is a mean across everyone randomized to the top dose, adherent or not [P1]. Some people lost far more, some far less. Anyone presenting it to you as “you will lose a fifth of your body weight” rather than “this is what happened on average in a trial” is rounding a statistic into a promise, and that’s not how any of this works.
Trick two: they skip the ladder and sell you the summit. Nobody starts at 15 mg. The dosing is a deliberate climb, low dose first, stepped up gradually, specifically to keep side effects manageable [P2]. The headline trial numbers describe where people land after months of escalation, not where anyone begins. If a seller lets you picture yourself jumping straight to the big number with none of the climb, that omission is doing work for them, not for you.
Trick three: they never mention the side effects have a pattern. The common adverse reactions are gastrointestinal, nausea, diarrhea, vomiting, constipation, and they cluster hardest around dose increases [P2]. That’s manageable information if someone tells you in advance. It’s a nasty surprise if you find out mid-injection from a seller who never brought it up.
Trick four, and this is the one that actually worried me: they skip the boxed warning entirely. Tirzepatide carries the FDA’s most serious warning classification because of thyroid C-cell tumors seen in rodent studies. It is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2 (MEN 2) [P2]. The label also flags acute pancreatitis and gallbladder problems, and it flags something almost nobody talks about: tirzepatide can reduce how well oral contraceptives work, which is why the label advises a barrier method, or switching off the pill, for four weeks after starting and after every dose increase [P2].
None of that is a reason to panic about the drug. It’s a reason to be furious at anyone who sells it to you without asking a single one of those questions first. A no-prescription vial doesn’t come with somebody checking your family history against that thyroid warning. It doesn’t come with somebody telling you about the birth control interaction before you find out the hard way. The molecule isn’t the risky part here. The missing screening is.
The legitimate route
This is the only place I’ll point you toward an actual door to walk through, because the contrast is the whole point of everything above. The label assumes, on every page, that a clinician is standing between you and the prescription. A licensed telehealth provider such as FormBlends is what that assumption looks like when someone actually builds a service around it: a licensed clinician reviews your history, checks you against the contraindications, including the thyroid history question that should worry anyone buying this blind, and only then does a prescription get written, filled by a licensed pharmacy, with follow-up attached. There’s nothing to click, buy, or check out here. That’s deliberate. The point isn’t to sell you anything. It’s to show you what “someone actually checked” looks like next to “a vial showed up.”
What I’d tell you if you only read one paragraph
The trial result is real: 20.9% average weight loss at 72 weeks on the top dose, against 3.1% on placebo [P1]. The mechanism is documented pharmacology, not marketing copy [P3]. The dosing is a ladder for a reason, and the side effects mostly show up while you’re climbing it [P2]. The boxed warning and the contraceptive interaction are written into the label precisely because someone is supposed to check them against you specifically, before you start [P2]. The question was never whether tirzepatide works. It was always whether the person handing it to you bothered to check if it’s safe for you. A checkout page will never answer that. A clinician will.
Questions people keep asking me about this
How much weight did people actually lose in the trial, and can I trust that number?
Yes, you can trust it, because it’s the conservative version. In SURMOUNT-1, mean weight loss at 72 weeks ran about 15.0% at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg, versus roughly 3.1% on placebo [P1]. That’s the treatment-regimen figure, meaning everyone randomized gets counted whether or not they stuck with the drug perfectly, which is why it’s the honest number and not the flattering one. It’s also an average, so don’t let anyone sell it to you as a personal guarantee.
Why does this drug outperform older weight-loss medications?
Because it works two levers instead of one. It’s a dual agonist, activating both the GLP-1 receptor that older drugs use and a second receptor called GIP that most of them don’t touch [P3]. Together they push more glucose-dependent insulin release, slow how fast your stomach empties, and dial down appetite [P3]. That’s pharmacology from the reference literature, not a marketing claim.
Why doesn’t anyone start at the highest dose if that’s where the big numbers come from?
Because the schedule is built as a gradual climb specifically to keep side effects tolerable [P2]. The 20.9% figure describes the maintenance dose people reach after escalating, not a starting point. The common side effects, nausea, diarrhea, vomiting, constipation, are worst around dose increases, and rushing the ladder is usually why people say they “couldn’t tolerate” the drug [P2].
What’s the boxed warning, and why does it matter so much to me?
It’s the FDA’s most serious warning category, applied here because of thyroid C-cell tumors seen in rodent studies. The drug is contraindicated if you or your family have a history of medullary thyroid carcinoma or MEN 2 [P2]. The label also flags pancreatitis and gallbladder issues as risks worth watching for. This is exactly the information a no-prescription seller has zero incentive to raise with you.
Does it really mess with birth control?
Yes, and it’s easy to miss. The label states tirzepatide can reduce how well oral hormonal contraceptives work, and advises using a barrier method or switching to a non-oral method for four weeks after starting and after every dose increase [P2]. It’s a small line in a long label, and it’s exactly the kind of detail that disappears when there’s no clinician reading it with you.
What’s actually different between buying this online with no prescription and going through a telehealth provider?
Who catches the mistakes. Skip the prescription step and the thyroid screening, the dose ramp, and the birth control warning all become your job, with none of the training to do it. A licensed telehealth provider such as FormBlends puts a clinician back into those decisions: your history gets reviewed, the contraindications get checked, a prescription follows only if it’s appropriate, and a licensed pharmacy fills it with follow-up built in. Same molecule. Completely different safety net around it.
References
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity. New England Journal of Medicine, 2022. PMID 35658024. Mean weight change at 72 weeks roughly 15.0% (5 mg), 19.5% (10 mg), 20.9% (15 mg) versus 3.1% placebo, treatment-regimen estimand. https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
- Tirzepatide (Zepbound) FDA-approved label, DailyMed. Boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2; warnings include acute pancreatitis and acute gallbladder disease; oral hormonal contraceptive interaction with advice to add a barrier method or switch to a non-oral method for 4 weeks; most common adverse reactions are gastrointestinal. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=487cd7e7-434c-4925-99fa-aa80b1cc776b
- Farzam K, Patel P. Tirzepatide. StatPearls, NCBI Bookshelf. Dual GIP and GLP-1 receptor agonist, 39-amino-acid GIP analog; increases glucose-dependent insulin secretion, slows gastric emptying, reduces appetite.
Tirzepatide is an FDA-approved medication (Zepbound, Mounjaro).
What exactly is tirzepatide and how does it work?
It’s a synthetic peptide built to mimic two gut hormones at once, GIP and GLP-1, which is the “dual agonist” bit you’ll hear tossed around. Both hormones normally show up after you eat. Together they tell your pancreas to release insulin, slow down how fast food leaves your stomach, and signal your brain that you’ve had enough. Hitting two receptors instead of one is the likely reason the weight-loss numbers look so much bigger than the older single-hormone drugs.
Is tirzepatide a GLP-1, and what does that mean for Mounjaro versus Zepbound?
It’s partly a GLP-1 receptor agonist, but calling it just that sells it short. It also activates GIP receptors, something older GLP-1 drugs like semaglutide don’t do. Mounjaro and Zepbound are the same molecule under two names. Mounjaro has FDA approval for type 2 diabetes, Zepbound for chronic weight management. What’s in the pen doesn’t change between them.
What side effects should I actually expect, and do they fade?
Nausea, diarrhea, vomiting, and constipation are the ones that show up most, and they cluster hard around dose increases. For most trial participants they were mild to moderate and eased within a few weeks of holding steady at a dose. A small share of people stopped treatment over GI symptoms. Smaller meals, skipping the heavy, fatty food, and not rushing the escalation schedule all seem to make the early weeks more bearable.
How does it stack up against semaglutide?
There isn’t much true head-to-head data yet, so any comparison is reading across two separate trials, which has limits. With that caveat: tirzepatide’s phase 3 trial showed average losses from roughly 15 to 21 percent at the highest doses, while semaglutide’s landmark trial landed around 15 percent at its top dose. Tirzepatide looks ahead on average, but individual responses vary a lot, and cost, access, and how well you tolerate it matter just as much as the headline percentage. If you’re looking at a compounded version, a provider like FormBlends works under a model where a prescriber is actually monitoring your dosing rather than leaving you to self-manage.